
Does your child often ask people to repeat themselves? Does he/she have problems with speech and language? Do you often find him/her intently watching others and trying to imitate their actions? Have you noticed how they don’t react even when you call them out loud…
This can be due to hearing loss in your child. As difficult as it may sound to come to terms with it, but it is not that unheard of for a child to suffer from hearing loss.

Hearing loss is not restricted by age – newborn babies, infants, and growing children are all equally susceptible to the disorder. In fact, it is possible to screen infants for hearing loss, within 24-48 hours after birth.
Dealing with hearing loss in children can be particularly taxing – While you are constantly trying to overcome your emotions and come to terms with it. It is taxing for the children too since they are not mature enough to bear the emotional burden of not being able to communicate. Being affected by hearing loss during their formative years, could also have an adverse effect on their confidence. To be able to cope with these challenges, it is necessary to understand why hearing loss strikes so early and how it can be treated.
To know if your child could be suffering from some form of hearing loss, here are some of the symptoms you will need to look out for.
Symptoms Of Hearing Loss In Children and Infants:

To identify the symptoms of hearing loss in infants can be quite a challenge. One way to determine if your child’s hearing is developing appropriately is by monitoring certain speech and hearing milestones. Although these milestones may not be the same for all children, they can be broadly trusted to reveal problems.
From birth to about 4 months, your infant should:
- Be startled by loud sounds
- Wake up or stir at loud sounds
- Respond to your voice by smiling or cooing
- Calm down at familiar voices
From 4 months to about 9 months, your infant should:
- Smile when spoken to
- Turn its head toward known sounds
- Make babbling noises
- Notice and respond to toys that make sound
- Understand certain motions of the hand
From 9 months to about 15 months, your infant should:
- Make various babbling noises
- Understand basic requests
- Respond to its name being called out
- Repeat some simple sounds
- Use its voice to get attention
From 15 months to about 24 months, your infant should:
- Point to body parts when asked
- Name common objects
- Listen to rhymes and songs with visible interest
- Use simple words
- Point to familiar objects you name
- Follow basic commands
For older children who acquire hearing loss, here are some of the things to watch out for:
- If he/she has difficulties understanding what people around him/her are saying
- If he/she speaks differently as compared to the other children of the same age
- If he/she doesn’t respond to his/her name being called out
- If he/she frequently misunderstands questions or responds inappropriately to them
- If he/she insists on turning up the TV volume or sits very close to the TV to hear clearly
- If he/she develops academic problems at school/college suddenly
- If he/she has speech or language problems
- If he/she intently watches others, to imitate their actions
- If he/she constantly complains of earaches or noises in the ears
- If he/she has trouble comprehending conversations over the phone or keeps switching ears while conversing over the phone
- If you hear him/her saying ‘what?’ or ‘huh?’ several times in a day
While hearing loss is usually considered to be a disorder that can only strike ‘older people’, it can be congenital too. Let’s take a look at some of the causes for hearing loss in children.
Causes Of Hearing Loss In Children:
Hearing losses in children can be sensorineural, conductive or mixed. Here are some of the known causes of hearing loss in children.

1. Congenital Hearing Loss:
Congenital hearing loss means that it was present in the infant at birth. It can be caused by both, genetic as well as non-genetic factors.
Non-Genetic Factors:
Non-genetic factors that might cause congenital hearing loss in children include:
- Birth complications, owing to serious infections, lack of oxygen or the requirement of a blood transfusion.
- Ingestion of life-sustaining drugs for respiration, in case of a premature birth.
- A nervous system or brain disorder.
- Use of ototoxic medication by the mother during the pregnancy term.
- If the mother had an infection during the pregnancy term.
- Maternal diabetes.
- Drug/alcohol abuse or smoking by the mother during the pregnancy term.
Genetic Factors:
Genetic factors that might cause congenital hearing loss in children include:
- Autosomal recessive hearing loss: In this case, neither parent has a hearing loss, but each parent carries a recessive gene that gets passed on to the child.
- Autosomal dominant hearing loss: In autosomal dominant hearing loss, one parent carrying a dominant gene for hearing loss passes it onto the offspring. This parent may or may not have hearing loss, but he or she might have other symptoms or signs of a genetic syndrome.
- Genetic syndromes: These include Usher syndrome, Treacher Collins syndrome, Waardenburg syndrome, Down syndrome, Crouzon syndrome and Alport syndrome.
2. Acquired Hearing Loss:
Children can acquire hearing loss, long after birth, owing to the following reasons:
- A perforated eardrum (a hole or rupture in the thin membrane that separates the ear canal and the middle ear.
- Otosclerosis (abnormal growth of bone near the middle ear) or Meniere’s diseases, both progressive disorders.
- Infections like meningitis, measles, mumps or whooping cough.
- Ingestion of ototoxic medications.
- A serious head injury.
- Exposure to loud noise, causing noise-induced hearing loss.
- Untreated or frequent otitis media (inflammatory diseases of the middle ear).
- Exposure to secondhand smoke.
3. Transient Hearing Loss:
Transient or fluctuating hearing loss in children is also detrimental to speech and language development. Transient hearing loss can be caused by otitis media, more commonly known as a middle ear infection. This type of infection is very common in children because of the Eustachian tube position during childhood. The Eustachian tube, which allows for air pressure equalization between the middle ear and the nasopharynx, is smaller and more horizontal during development. Thus, it is susceptible to blockage by fluids or large adenoids.
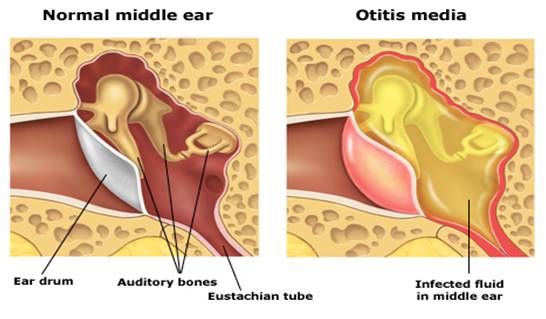
Transient hearing loss due to an ear infection can occur when fluid inhibits the vibrations of the tiny middle ear bones, making efficient sound transmission difficult. Normally, this type of hearing loss is temporary and eventually resolves itself. However, frequent, untreated middle ear infections can cause cumulative damage to the bones, eardrum or auditory nerve, creating a permanent, sensorineural hearing loss.
If your child exhibits any or all of the symptoms mentioned before, it is ideal to first take him or her to your family doctor, who might refer you to a pediatric audiologist for further tests. Audiologists have several painless and noninvasive tests on children as young as 6 months old.
Once the tests have been conducted, and the hearing loss is confirmed, the audiologist will chart out an appropriate treatment plan. Let’s take a look at some of the treatments usually suggested for children with hearing loss.
How Should I Confirm Whether My Child Has Hearing Loss?
Determining hearing loss in children is more challenging as compared to adults. Adults are capable of responding to sounds or tones presented to them at the time of evaluation. However, very young children, or children who have not yet developed speech, or children who might have other disorders, require a detailed battery of tests to establish the type and degree of hearing loss. Once identified, the course of treatment for hearing loss in children can best be determined with evaluations which help localize the problem, determine the extent of the problem and to find out what the level of hearing loss might be across frequencies.
Hearing in infants can be tested using two different methods: the auditory brainstem response (ABR) evaluations or the otoacoustic emission (OAE) measures. Both tests are accurate, noninvasive, automated, and do not require any observable response from the infant. Let’s take a detailed look at the tests.
1. OAE (Oto-Acoustics Emissions):
This test should universally be performed on all newborn babies to ensure early intervention. This test can help identify any kind of dysfunctioning of the outer hair cells. In case the infant fails this test, it is recommended to repeat the test again in a few months and if recommended, conduct a BERA test.
2. BERA (Brain Evoked Response Audiometry):
Also known as the Auditory Brainstem Response (ABR) test, this is a helpful tool in determining a child’s ability to hear. The test uses a special computer to measure the way the child’s hearing nerve responds to different sounds. The test is usually performed with the child in a state of deep sleep. In slightly older children or hyperactive children, there might be a need for sedation.
3. Tympanometry:
This tests how the eardrum and middle ear are working. This test is important because fluid or other problems in the middle ear can affect hearing. During tympanometry, a small earphone is placed in the ear canal and air pressure is gently changed. A tympanogram is a graph of the test results, which can help identify the following:
- Fluid present in the middle ear
- Holes in the eardrum
- Eustachian tube problems
- Presence and function of pressure equalization or tympanostomy tubes
If the tympanogram is not normal, babies or young children may be referred to their doctor for medical treatment.
4. Auditory Steady State Responses (ASSR):
ASSR testing is another electrophysiologic measurement of a baby’s hearing. The results of this test may provide more frequency-specific threshold information for infants who have severe to profound hearing losses. This enables the audiologist to have more precise data to proceed with hearing aid fittings or determining cochlear implant candidacy. Like the ABR assessment, infants over 6 months of age may need to be sedated for ASSR testing.
5. Behavioral Audiometry:
As a child matures and is able to provide hearing results behaviorally, hearing information can be plotted with even greater specificity. During audiometric testing, the audiologist finds the lowest intensity level (threshold) at which a child can detect sound at different frequencies. From this information, a graphic representation of the hearing loss called an audiogram, is created. Based on the audiogram, the hearing loss will typically be classified as mild, moderate, moderately severe, severe, or profound.
Treatment For Hearing Loss In Children:
Based on the severity and type of hearing loss, the audiologist can recommend any of the treatment procedures mentioned below:
1. Hearing Aids:
Hearing aids are devices that help children with hearing loss hear clearly again. Many solutions for children include special coverings and other accessories to ensure that young children don’t remove or misplace their hearing aids. There are several types of hearing aids to choose from, based on the preferences of the child, as well as the kind of environment he/she lives in.
2. Cochlear Implants:
Cochlear implants are surgically implanted devices that directly stimulate the auditory nerve in the inner ear with electrical stimulation. Cochlear implants have an external device, and many companies make kid-friendly devices that can be held on with a soft headband. Cochlear implants work for infants and children who cannot benefit from hearing aids.
3. Speech Therapy:
For children whose hearing loss has affected their speech might need speech and language therapy after getting hearing aids or a cochlear implant. Speech therapy may be required to treat speech disorders such as:
- Articulation disorders: difficulties producing sounds in syllables or saying words incorrectly to the point that listeners can’t understand what’s being said.
- Fluency disorders: problems such as stuttering, in which the flow of speech is interrupted by abnormal stoppages, repetitions (st-st-stuttering), or prolonging sounds and syllables (ssssstuttering).
- Resonance or voice disorders: problems with the pitch, volume, or quality of the voice that distract listeners from what’s being said. These types of disorders may also cause pain or discomfort for a child when speaking.
- Dysphagia/oral feeding disorders: these include difficulties with drooling, eating, and swallowing.
4. Assistive Listening Devices:
Assistive listening devices such as FM (Frequency Modulated) systems are discreet and work well in a classroom situation in conjunction with the child’s hearing aid or cochlear implant. FM systems transmit sound from one person to another over distance overcoming the effects of noise, reverberation, and distance. This helps to overcome the poor acoustics of classroom settings or other venues with lots of background noise. Essentially, the teacher wears or has a discreet microphone in front of him or her that transmits his or her voice directly to the child’s hearing aids or cochlear implant.
Treating hearing loss is not the last step, especially when it comes to children. We know how difficult it is for an adult to adjust to devices like hearing aids and cochlear implants. With children, it becomes a matter of ensuring that their confidence doesn’t bear the brunt of their hearing loss. Here are some ways you can make it easier for your hearing impaired child.
Coping With Hearing Loss In Children:

Coping with hearing loss in a child needs continuous engagement and focus. Here are some ways you can make sure that your child is able to deal with the hearing loss, as well as the use of hearing aids or other devices.
- Try to change your child’s perception of hearing aids. Opt for colourful ear molds and ear wraps to keep the hearing aid in place. Make having a hearing aid seem as fun as possible.
- Help your child adapt to the hearing aid. Try to draw their attention away from the hearing aid.
- Talk to your child as much as possible, to make him/her ‘want’ to use the hearing aid.
- Celebrate small successes – strive for full-time hearing aid use, but keep in mind that your child may not want to wear them throughout the day.
- In the case of cochlear implants, choose the device your child will be comfortable with.
- Work closely with the audiologist. Audiologists are experienced in dealing with a lot of children with the same disorder as your child. It is easier to find solutions to challenges if you use that experience to your advantage.
- MOST IMPORTANTLY – Ensure they don’t feel any different. Let them be confident of themselves.
It isn’t easy dealing with children who have hearing loss. But, with timely diagnosis and careful treatment, your child can live a normal and healthy life!
If you suspect your child could be suffering from hearing loss, – Get in touch with Centre For Hearing! We offer the expertise of over 50 RCI certified audiologists and comprehensive diagnostic facilities.
Call us today for a FREE Consultation on +91 9811227492